People consider anxiety as a mood disorder, a DSM-5* psychiatric diagnosis. After brain injury, it’s much more complicated than that. The 21st century calls for basing our understanding of anxiety in neuroscience not on the DSM’s* subjective symptom listing.
On 29 April 2013, Thomas Insel, then the Director of the National Institute of Mental Health in the USA, declared that the NIMH will be reorienting away from the traditional Diagnostic and Statistical Manual of Mental Disorders (DSM-5). The NIMH essentially declared the categories of symptoms for brain issues no longer useful nor wanted. As Insel wrote, “symptom-based diagnosis, once common in other areas of medicine, has been largely replaced in the past half century as we have understood that symptoms alone rarely indicate the best choice of treatment.”
Busy Brain
Busy brain describes what’s happening in an injured brain. Instead of oscillating at their normal brainwave frequencies, neurons oscillate at much higher frequencies, the frequencies associated with anxiety. And not just normal anxiety, but anxiety that’s like a hamster wheel that never stops and the hamster running in it has drunk ten thousand caffeine-laced drinks. It’s like the neurons go bananas and you cannot stop the round-and-round thought that keeps your brain busy with it, excluding all other thoughts. It’s not psychological. It’s neurological. You cannot physically stop it on your own.
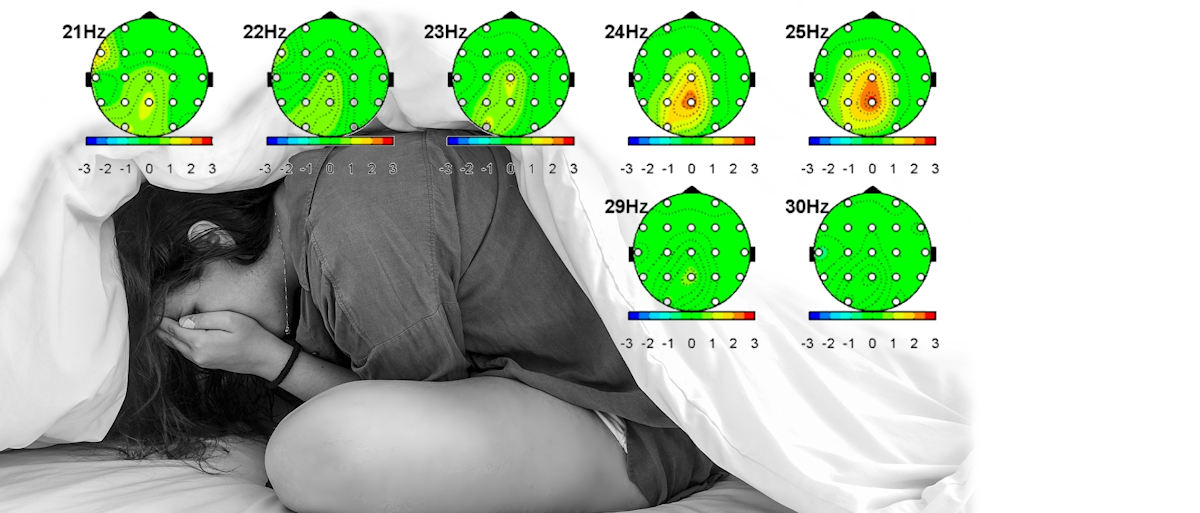
Brainwave frequencies associated with busy brain range from 21 to 35 Hz in the beta category. The entire brain may not be producing these frequencies; they may be localized to certain areas. But the subjective feeling is the same. Pinpoint diagnostics with qEEG reveal where Busy Brain is located and the specific brainwave frequencies that are in excess. To permanently retrain the brain not to produce Busy Brain is like peeling an onion. You begin with the widest range and narrow it down over time; for example, begin reducing 21 to 35 Hz at CZ; narrow down over months or years to 24 to 28 Hz. As the disinhibiting brain training progresses, anxiety and related irritability drops or disappears.
Neural Chaos
The adage neurons that fire together wire together assume that neurons are oscillating in harmony like they’re supposed to. After brain injury, neurons begin oscillating out of their natural alpha brainwave frequency and out of harmony. If you could hear it, it would sound like a cacophony that sends your hands to your ears to protect yourself from the awful sound. In contrast, neurons firing in harmony would sound like a hum.
Neurons that fire individually, producing neural chaos, impede function. You cannot do much of anything when neural chaos exists inside your skull. You cannot process sensory information, conversations, events, facial expressions, ideas, and so on with a brain in chaos. That inability leads to confusion, and the neural chaos also manifests as anxiety. It’s like a two-fer. Neural anxiety creating confusion.
Re-establishing the disrupted alpha rhythm in the corticothalamic loop (which connects the thalamus to the cerebral cortex and cortex to thalamus in a loop) will noticeably reduce anxiety and agitation.
anxiety is rooted in injured neurons
Confusion
Brain injury manifests in many ways. Commonly, injured neurons and neural networks damages cognitions. Damage may include loss of concentration, distortion of perceptual abilities, loss of memory both short term and long term as well as working memory, loss of affect, loss of identity, and so on. In addition, brain injury slows processing down significantly in everyone.
Note: A slowed processing speed is perceived as normal within the injured person’s mind, but it looks very slow from the outside.
Gravity, a Star Trek Voyager episode, demonstrates this perceptual difference well. Tuvok, Paris, and The Doctor crash land on a planet that exists in accelerated time. Voyager remains in normal time. To Voyager, the planet is spinning like a vortex. To the three men, time appears normal on the planet but very very slowed down with Voyager. Voyager is like the person with the brain injury; Tuvok, Paris, and The Doctor like the uninjured.
Another way to think of it: For the person with brain injury, trying to participate in a conversation or make a decision is like watching a show sped up. Voices squeak rapidly in helium-high frequencies with words running into and over each other at 200kph. It’s kind of funny, right? You’re smiling and chuckling right now — because of the sound of it. Who cares what the words are! Now imagine you have to care. Everyone around you understands the words themselves except you. Everyone expects you to keep up with the squeaky voices and to comprehend the rapid words in real time. You’re the only one who cannot make out the words, process them in real time, and respond. You see people laughing or nodding and you cannot participate with them. You think: It’s impossible! Who can make out the words?! They think: What’s wrong with them?! They become exasperated with you while confusion reigns in you.
Slow processing creates confusion because you can’t comprehend in real time, whether it’s conversation, traffic lights, picking out apples, someone yelling at you, working out a tip on a meal, reading a public transit map. You see others having no difficulty, you don’t understand why it’s so hard for you, and you’re given no time to process. Confusion arises, then anxiety, then panic.
Impaired perception also creates confusion. Why is someone laughing or smiling? You can’t perceive the humour. Damaged cognitions begin to intersect: loss of humour plus impaired perception equals greater confusion. Throw in slow processing, and anxiety ratchets up and irritability sets in.
Confidence Loss
Confidence in one’s competencies affects anxiety in a positive way. The opposite is true as well: when brain injury suddenly and inexplicably yanks away your talents and skills, when you begin to fail in areas you either performed automatically or well, your confidence falters. You begin to be anxious about not knowing how to do something you used to do easily; you become confused about failing them then anxious then resentful at being asked to do something you cannot. And that anxiety may expand into other areas — for if you cannot read books you used to find easy, if newspaper articles become weirdly incomprehensible, when comic strips all of a sudden make no sense, then what other things will vanish from your competencies? That creates anxiety.
Summing Up
In other words anxiety is rooted in injured neurons and neural networks. It’s compounded by intolerant people who won’t accommodate damaged cognitions and ratcheted up by failure to restore competencies after brain injury damages them.
*DSM-5 is the Diagnostic and Statistical Manual of Mental Disorders, fifth edition, that psychiatrists use as their bible. I personally think it’s an inappropriate tool for brain injury. Objective diagnostic methods are more accurate, revealing, and actionable.
The graphics in the Featured Image at the top show brainwave prevalence in the frequencies indicated at the top left of each “head.” Yellow areas indicate higher than the norm and tell the specialist that these frequencies in those locations need to be reduced.