Neuropsychology tests or neuropsychological test battery or assessment come in two versions: online or pencil and paper. They can take from one hour to all day. The pencil-and-paper one comprises multiple components, any one of which may or may not be included in a test battery so that every test may not be exactly the same, even though some components will appear in every test. It may include components done on the computer. That means for someone like me who had about eight of them, two of them online, over the course of 17 years, each test battery contained familiar components and unfamiliar ones.
The Tradition
From the client perspective, the pencil-and-paper test comprises a human sitting across from you and
- asking you questions and noting down your answers on a computer sheet or handwriting them, sometimes with a stopwatch in hand, sometimes not;
- having you look at and pick out one drawing out of four possible ones that matches a drawing on a flipboard;
- having you manipulate red-and-white plastic blocks to match increasingly more difficult red-and-white drawings on a flipboard;
- asking you to look at drawings of boxes opened up to be flat in 2D in order to find the one that matches a drawing of a box in 3D;
- reading you stories then asking you questions about them at the time as well as later;
- times you during some of the components with a visible stopwatch (even if they keep it in an unobtrusive place, you can still see them starting it);
- asking you to memorize a series of numbers or words then asking you to recall them forwards and backwards immediately after as well as later;
- asking you to manipulate pegs in a board, first with your right hand then with your left;
- and much much more.
Sometimes the test battery will include an IQ test. I wrote about my experience in Concussion Is Brain Injury: Treating the Neurons and Me.
The Online Version
The online test differs greatly from the pencil-and-paper one. You do the entire online test alone in a room. There is no possibility of a brain supporting your brain as the computer tests you. As I’ve written before, brains support brains. That’s why a person with brain injury may be able to read easier when sitting next to someone than when by themself, for example.
You can do the online test at home when you’re fresh or at the clinic and in a quiet place. The pencil-and-paper test battery ought to be done in a quiet place as well, but I’ve had one done in a busy area.
the brain functions in milliseconds and microvolts
From the client perspective, the online test
- asks questions similar to the pencil-and-paper one except that you can see the questions and choices;
- shows you choices in letter sizes easily readable;
- times you without you necessarily realizing it;
- has you do finger tapping tests to measure reaction time to the millisecond, a real-time assessment of your reaction times (humans cannot measure reaction times as well as a computer);
- is short;
- is done as part of a battery of objective tests, not relied on alone as a diagnostic tool.
Elbert W. Russell wrote in The Scientific Foundation of Neuropsychological Assessment:
“Neuropsychological test batteries have traditionally attempted to fashion complete coverage by selecting tests that cover all of the various anatomical areas of the brain. This approach has been used from the time that it was realized that different areas of the brain have different functions. A proper selection of tests helps determine the localization of the damage (Reitan, 1964). In addition, the diagnosis of a pathology is dependent on the areas that are impaired.”
ScienceDirect, Neurospychological Test Battery
The writers for The Handbook of Psychological Assessment (Fourth Edition) noted:
“Neuropsychological test batteries must of necessity be administered to brain-damaged patients, many of whom may have severe physical disability, cognitive impairment, or a combination of the two. Thus, stimulus and response characteristics of the tests themselves, as well as the stimulus characteristics of the test instructions, become exceedingly important considerations. Neuropsychological test material should, in general, be constructed with salient stimuli that the patient can readily see or hear and understand. Material to be read should not require high levels of literacy, nor should grammatical structures be unduly complex.”
ScienceDirect, Neuropsychological Test Battery
Are They Worth Doing?
Neuropsychological tests are a complete waste of time.
I see your outrage at my statement.
If you’re a specialist who uses them, you’ve decided I’m ignorant. If you’re a person with brain injury, you either fully agree or are outraged because the cognitive dissonance of going through an entire hellacious day of endless questions and physical manipulations and stopwatches resulting in catatonic-like fatigue cannot end up being a waste of time.

I came to this conclusion after enduring several of these tests that lead to misdiagnosis, no effective treatment, or no options for recovery.
The brain functions in milliseconds and microvolts; testing it requires measuring at that level of precision and accuracy.
Neuropsychological test batteries cannot measure neuronal function at the speed at which they operate. Neurons fire and recover fast.
assessing brain damage requires precision and accuracy
Not a single neuropsychological assessment lead to an accurate assessment of my brain damage. How can they when they don’t measure the cellular processes leading to cascading damage nor the hidden brainwave changes measurable only by qEEG or evoke potentials and specialized scans?
More importantly, not a single assessment had any effect on my treatment regimen: not on choosing my treatments, not on changing them, not on seeking better treatments. Not a single assessment lead to any amount of recovery.
The online neuropsychological testing I did as part of an overall battery of objective qEEG and computer testing had interesting results, weren’t as affected by my IQ as the pencil-and-paper ones, and supported the results from the other tests, but the qEEG, evoke potentials, and IVA tests are what drove my treatment protocols.
If you have a high IQ, even one that brain injury dropped significantly, traditional neuropsychological assessments may not reveal the true extent of the damage, probably because you’re able to mask the damage during symptom-based assessments, other than components like putting pegs in holes.
Results are usually couched in descriptive terms instead of precise location-specific measurements.

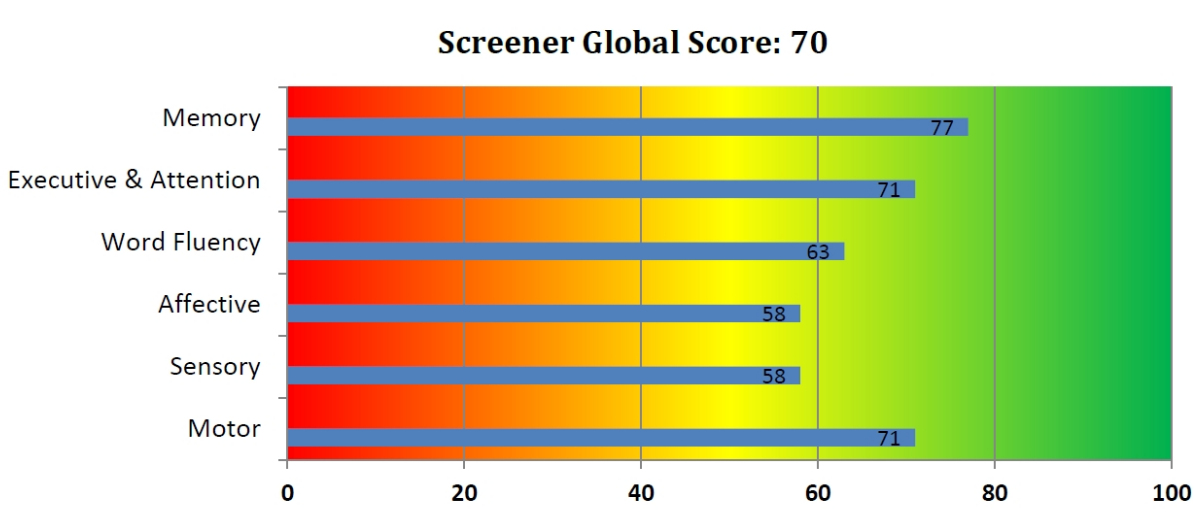
I found the pencil-and-paper tests don’t measure real-world memory loss. For example, the testor would read a story to me then assumed that since I recalled it within the testing timeframe that my long-term memory was intact, yet I’d regularly forget major events like a family cat dying, what I did the day before, whether I brushed my teeth, and so on. Memory tests comprising numbers or words don’t capture memory issues in a person who retains pattern recognition. I’d rather see memory tests designed around real-world issues, requiring information and personal historical knowledge from family and friends that become part of the test. The online test was closer to the mark (see image above).
Reading is not tested properly in these tests, from my experience. Reading alone requires about four hours to test. See the Reading section.
These tests have in-built biases. Stopwatches add the assessor’s reaction time to the testee’s time. I easily aced the never-seen-before story memory tests because I had read these stories for years in my childhood and adolescence. Canadians may not have seen those stories, but with my British and educational background, I had. Didn’t matter to the tester. It was part of the test, supposed to be new, so on we went.
I will concede the online test measuring reaction time is useful. That’s because time is an objective measure a computer can assess accurately down to the millisecond and because reaction times tell the specialist something about brain damage. I will also concede that the TOVA, which can be part of a traditional neuropsychological test battery, is useful to measure the variables of attention, but that’s because it’s conducted by a computer with no one else in the room. (I wrote a description during which my brain underwent spontaneous improvement.) The principle here is the test is objective, conducted without the possibility of introducing either human error or human support through proximity, and measures function not symptom.
The Stroop test online measures how long your brain processes a task when given conflicting information at the same time. The Stroop test will show slowed processing speed, and if you had a baseline before a concussion, it may reveal the change from the injury. However, evoke potentials and qEEG give a precise picture of processing speed within the brain and between the brain and the outside world. Administering the Stroop test during a qEEG recording will show both what the brain is doing and how you as the person functions as the test becomes increasingly faster and harder.
Some of these tests are kind of fun to do, like the red-and-white block manipulations and the Stroop Test. You can find many of these tests online and have fun doing them.
I was told that test results less than 2 years apart will be biased because of the effect of familiarity. Even if you cannot consciously remember every part of the assessment, enough familiarity will remain to bias your scoring upward.
Recommendation
My recommendation when you’re asked is to demand the online one as part of an overall objective assessment that includes qEEG. If that’s not possible or you feel obligated to do the all-day battery of in-person pencil-and-paper, then require that it be split up into two-hour blocks over several days and weeks so that you have enough time to recover and won’t suffer with intense fatigue and migraine for days or a week after. There is nothing that says splitting it up will affect the results. Doing so will minimize the deleterious effect on functionality as well as provide some feeling of control. The online assessment can be done when you have good energy as you can do it at home in a quiet place or at the clinic after a rest, and it’s short.
If you’re looking for an accurate measure of your brain damage and/or for a diagnosis that will inform treatment, these tests will not provide the information that you seek. At best, they’ll support the results of objective diagnostic tests.